
Injuries of the Larynx and Trachea
The larynx and trachea may be injured by:
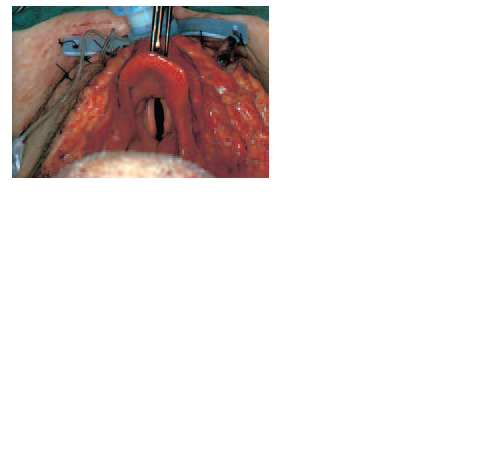
1 penetrating wounds, e.g. gunshot or cut throat injuries (Fig. 32.1);
2 blunt trauma, especially from road traffic accidents;
3 inhaled flames or hot vapours;
4 swallowed corrosive poisons;
5 endotracheal tubes and inflatable cuffs.
MANAGEMENT
The diagnosis of laryngeal trauma is often missed amid other serious injuries,
but should always be suspected when injury to the neck has occurred.
Cricotracheal separation may not cause immediately obvious signs
but may lead to asphyxia. Fractures of the larynx will produce hoarseness
and stridor, and tracheostomy may be needed urgently. In cases of cut
throat, it may be possible to intubate the larynx through the wound, prior
to formal tracheostomy and laryngeal repair. The two priorities of treatment
are:
1 to protect the airway by intubation or tracheostomy;
2 to restore laryngeal function by careful repair of the injury.
Laryngeal stenosis may result, despite repair of the larynx, and a permanent
tracheostomy is sometimes necessary.
124
Fig. 32.1 A self-inflicted cut
throat, giving a good view of
the anatomy.
Various manoeuvres for the correction of laryngeal stenosis have been
devised, most depending on widening the lumen with some form of skeletal
graft, such as rib cartilage or the hyoid bone.
INTUBATION
A particular problem is that posed by long-term endotracheal intubation of
patients on intensive care units. The avoidance of red rubber tubes and
awareness of the need to control cuff pressures have led to a reduction in
the incidence of stenosis, and with modern tube design, tracheostomy can
usually be postponed for 2–3 weeks. Once a problem mainly limited to adult
intensive-care units, there has been an increased incidence of subglottic
stenosis among very premature babies as a result of improved survival
rates, owing to the excellent care of neonatologists. Prolonged endotracheal
ventilation for broncho-pulmonary dysplasia and respiratory distress
syndrome has inevitably resulted in cases of laryngeal stenosis in tiny infants,
the care of whom is highly specialized and beyond the scope of this book.


Download Files
Course Material
- The Ear: Some Applied Anatomy
- Clinical Examination of the Ear
- Testing the Hearing
- Deafness
- Conditions of the Pinna
- Conditions of the External Auditory Meatus
- Injury of the Tympanic Membrane
- Acute Otitis Media
- Chronic Otitis Media
- Complications of Middle-Ear Infection
- Otitis Media with Effusion
- Otosclerosis
- Earache (Otalgia)
- Vertigo
- Facial Nerve Paralysis
- Adenoids
- The Tonsils and Oropharynx
- Tonsillectomy
- Retropharyngeal Abscess
- Examination of the Larynx
- Injuries of the Larynx and Trachea
- Acute Disorders of the Larynx
- Chronic Disorders of the Larynx
- Tumours of the Larynx
- Vocal Cord Paralysis
- Airway Obstruction in Infants and Children
- Conditions of the Hypopharynx
- Tracheostomy
- Diseases of the Salivary Glands
- Chapters 29
- Department Sargodha Medical College
- Teacher
Dr. Muhammad Khalil
