
Examination of the Larynx
The visualization of the larynx is obviously of paramount importance in
dealing with laryngeal disease, and several methods are available.
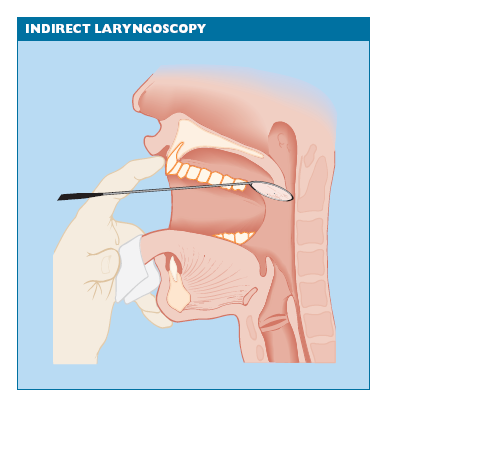
INDIRECT LARYNGOSCOPY
This is the most convenient method of examination but it requires instruction
and practice.
The patient protrudes his tongue, which is held gently between the examiner’s
middle finger and thumb (Fig. 31.1).The forefinger is used to hold
the upper lip out of the way and a warmed laryngeal mirror is introduced
gently but firmly against the soft palate in the midline. By tilting the laryngeal
mirror, the various structures shown in Fig. 31.2 can be inspected. Mobility
of the cords is assessed by asking the patient to say ‘EE’, causing adduction,
or to take a deep breath, which causes abduction. The beginner will often
see only the epiglottis, with a fleeting glimpse of the cords, but continued
practice will allow visualization of the larynx and hypopharynx in most
subjects.
In recording your findings, bear in mind that the image you see is
reversed. It is advisable to label your diagram L and R in case confusion with direct examination occurs.
FIBRE-OPTIC LARYNGOSCOPY
In some cases the patient will not tolerate indirect laryngoscopy, or the
view of the vocal cords is obstructed by an overhanging epiglottis. In these
cases, fibre-optic laryngoscopy makes examination possible without recourse
to general anaesthesia.The flexible fibre-optic instrument is passed
through the anaesthetized nose into the pharynx. It is then manoeuvred
past the epiglottis until the interior of the larynx is seen. Although the image
is smaller than that obtained by mirror examination, it allows inspection
of the cords during phonation and also enables a photographic record to
be made. The patient can even view his own larynx through a teaching
attachment.
DIRECT LARYNGOSCOPY
Under general anaesthesia, a laryngoscope supported by some form of suspension
apparatus is introduced into the larynx.With the aid of an operating
microscope, a superb binocular-magnified view of the larynx is obtained
and endoscopic surgery can be carried out with precision. This technique
also allows the use of a carbon dioxide laser for the treatment of such
lesions as papillomata and leukoplakia. Closed-circuit television, video or
still photography are simple to attach to the microscope for making a record of the findings


Download Files
Course Material
- The Ear: Some Applied Anatomy
- Clinical Examination of the Ear
- Testing the Hearing
- Deafness
- Conditions of the Pinna
- Conditions of the External Auditory Meatus
- Injury of the Tympanic Membrane
- Acute Otitis Media
- Chronic Otitis Media
- Complications of Middle-Ear Infection
- Otitis Media with Effusion
- Otosclerosis
- Earache (Otalgia)
- Vertigo
- Facial Nerve Paralysis
- Adenoids
- The Tonsils and Oropharynx
- Tonsillectomy
- Retropharyngeal Abscess
- Examination of the Larynx
- Injuries of the Larynx and Trachea
- Acute Disorders of the Larynx
- Chronic Disorders of the Larynx
- Tumours of the Larynx
- Vocal Cord Paralysis
- Airway Obstruction in Infants and Children
- Conditions of the Hypopharynx
- Tracheostomy
- Diseases of the Salivary Glands
- Chapters 29
- Department Sargodha Medical College
- Teacher
Dr. Muhammad Khalil
