
Facial Nerve Paralysis
Paralysis of the facial nerve is a subject of fascination to the otologist and
a cause of distress to the patient. Owing to its frequency and diversity of
aetiology, it is a matter of very considerable importance to workers in all
spheres of medical life.
The causes are numerous and are considered in Table 16.1.
DIAGNOSIS
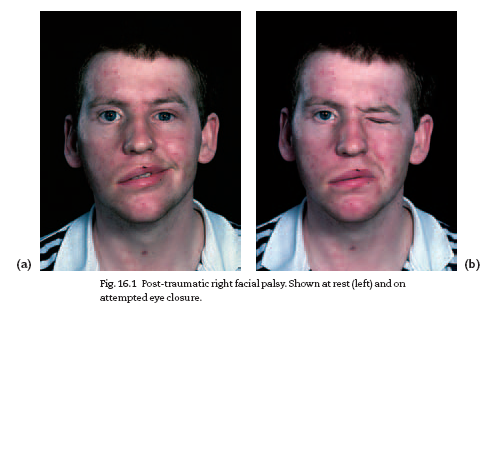
The patient presents with a varying degree of weakness of the facial muscles
and sometimes difficulty in clearing food from the bucco gingival sulcus as a
result of buccinator paralysis.
Facial asymmetry is accentuated by attempting to close the eyes tightly,
to show the teeth or to whistle (Fig. 16.1).
It is important to remember that in supranuclear lesions the movements
of the upper part of the face are likely to be unaffected as the forehead
muscles have bilateral cortical representation.Moreover, involuntary movements
(e.g. smiling) may be retained even in the lower face. A most careful
history and aural and neurological examination are essential, including attention
to such matters as impaired taste (lesion is above origin of chorda tympani),
hyperacusis with loss of the stapedius reflex (lesion is above nerve to
stapedius) or reduction of lacrimation (lesion is above geniculate ganglion).
Electrodiagnosis is used in the assessment of the degree of involvement
of the nerve and includes nerve conduction tests and electromyography.
A detailed description of the various tests is beyond the scope
of this volume, but their application is of value as a guide to prognosis and
management.
palsy (idiopathic facial paralysis)
Bell’s palsy is a lower motor neurone facial palsy of unknown cause, but possibly
viral. It is part of the group of idiopathic cranial mono-neuropathies.
Bell’s palsy may be complete or incomplete; the more severe the palsy,
the worse the prognosis for recovery. In practice, full recovery may be
expected in 85% of cases.The remainder may develop complications, such
as ectropion or synkinesis.
CAUSES OF FACIAL NERVE PARALYSIS
Supranuclear and nuclear
Cerebral vascular lesions
Poliomyelitis
Cerebral tumours
Infranuclear
Bell’s palsy
Trauma (birth injury, fractured temporal bone, surgical)
Tumours (acoustic neurofibroma,parotid tumours, malignant disease of
the middle ear)
Suppuration (acute or chronic otitis media)
Ramsay Hunt syndrome
Multiple sclerosis
Guillain–Barré syndrome
Sarcoidosis
Table16.1 Causes of facial nerve paralysis.
TREATMENT
Treatment of Bell’s palsy should not be delayed.
1 Prednisolone given orally is the treatment of choice, but only if started
in the first 24 h. In an adult, start with 80 mg daily and reduce the dose
steadily to zero over a period of 2 weeks.
2 Surgical decompression of the facial nerve is a matter of controversy:
some authorities decompress at an early stage: most do not advise
decompression.
3 Tarsorrhaphy may be needed to protect the cornea of the unblinking
eye.
4 In the rare event of recovery not taking place, cross-facial grafting or
hypoglossal–facial anastomosis may be carried out to restore symmetry to
the face.
5 Inward collapse of the cheek can be disguised with a built-up denture to
restore the contour.
Do not make a diagnosis of Bell’s palsy until you have excluded
other causes. If recovery does not take place in 6 months, reconsider
the diagnosis.
Ramsay Hunt syndrome
This is due to herpes zoster infection of the geniculate ganglion, affecting
more rarely the IX and X nerves and, very occasionally, the V, VI or XII.The
patient is usually elderly, and severe pain precedes the facial palsy and
the herpetic eruption in the ear (sometimes on the tongue and palate).The
patient usually has vertigo, and the hearing is impaired. Recovery of
facial nerve function is much less likely than in Bell’s palsy.
Prompt treatment with acyclovir given orally may improve the prognosis
and reduce post-herpetic neuralgia.
Facial palsy in acute or chronic otitis media
This requires immediate expert advice, as urgent surgical treatment is
usually necessary.
Traumatic facial palsy
This may result from fracture of the temporal bone or from ear surgery. If
the onset is delayed, recovery is to be expected but if there is immediate
palsy, urgent surgical exploration and decompression or grafting will be
required. Otological advice should be sought without delay


Download Files
Course Material
- The Ear: Some Applied Anatomy
- Clinical Examination of the Ear
- Testing the Hearing
- Deafness
- Conditions of the Pinna
- Conditions of the External Auditory Meatus
- Injury of the Tympanic Membrane
- Acute Otitis Media
- Chronic Otitis Media
- Complications of Middle-Ear Infection
- Otitis Media with Effusion
- Otosclerosis
- Earache (Otalgia)
- Vertigo
- Facial Nerve Paralysis
- Adenoids
- The Tonsils and Oropharynx
- Tonsillectomy
- Retropharyngeal Abscess
- Examination of the Larynx
- Injuries of the Larynx and Trachea
- Acute Disorders of the Larynx
- Chronic Disorders of the Larynx
- Tumours of the Larynx
- Vocal Cord Paralysis
- Airway Obstruction in Infants and Children
- Conditions of the Hypopharynx
- Tracheostomy
- Diseases of the Salivary Glands
- Chapters 29
- Department Sargodha Medical College
- Teacher
Dr. Muhammad Khalil
