
Deafness
Attention has already been drawn to the two major categories of
deafness—conductive and sensorineural. The distinction is easily made by
tuning fork tests, which should never be omitted.
CAUSES
There is no strict order in the list featured in Table 4.1, because the frequency
with which various causes of deafness occur varies from one community
to another and from one age group to another.Nevertheless, some
indication is given by division into ‘more common’ and ‘less common’
groups. Always try to make a diagnosis of the cause of deafness and start by
deciding whether it is conductive or sensorineural.
MANAGEMENT
The management of a number of specific conditions will be dealt with in
subsequent chapters but some general comments are appropriate.
deaf child
Early diagnosis of deafness in the infant is essential if irretrievable developmental
delay is to be avoided.The health visitor should screen all babies at
about 8 months of age and those failing a routine test must be referred to a
specialist audiological centre without delay for more thorough investigation.
Some babies are ‘at risk’ of deafness and are tested as soon after birth
as possible.They include those affected by:
1 prematurity and low birth-weight;
2 perinatal hypoxia;
3 Rhesus disease;
4 family history of hereditary deafness;
5 intrauterine exposure to viruses such as rubella, cytomegalovirus and
HIV.
The testing of babies suspected or at risk of being deaf is very specialized.
The mother’s assessment is very important and should always be taken seriously.
She is likely to be right if she thinks her child’s hearing is not normal.
Testing of ‘at risk’ babies in the neonatal period is now carried out in many
centres by the recording of otoacoustic emissions (see Chapter 3).
Conductive Sensorineural
More common
Wax Presbycusis (deafness of old age)
Acute otitis media Noise-induced (prolonged exposure to high
noise level, industrial deafness, chronic otitis
media disco music)
Barotrauma Congenital (maternal rubella, cytomegalovirus,
Otosclerosis toxoplasmosis, hereditary deafness,anoxia,
jaundice,congenital syphilis)
Injury of the tympanic membrane Drug-induced (aminoglycoside antibiotics,
aspirin, quinine, some diuretics, some beta
blockers)
Menière’s disease
Late otosclerosis
Infections (CSOM,mumps,herpes zoster,
meningitis, syphilis)
Less common
Traumatic ossicular dislocation Acoustic neuroma
Congenital atresia of the external Head injury
canal
Agenesis of the middle ear CNS disease (multiple sclerosis, metastases)
Tumours of the middle ear Metabolic (diabetes,hypothyroidism,
Paget’s disease of bone)
Psychogenic
Unknown aetiology
Sudden sensorineural deafness
Sudden sensorineural deafness is an otological emergency and should be
treated as seriously as would be sudden blindness. Immediate admission to
hospital should be arranged, as delay may mean permanent deafness.
Sudden deafness may be unilateral or bilateral and most cases are regarded
as being viral or vascular in origin. Investigation may fail to show a
cause and treatment is usually with low-molecular-weight dextran, steroids
and inhaled carbon dioxide. Bilateral profound deafness, especially if of sudden
onset, is a devastating blow and for this reason various organizations
exist to give advice and support.
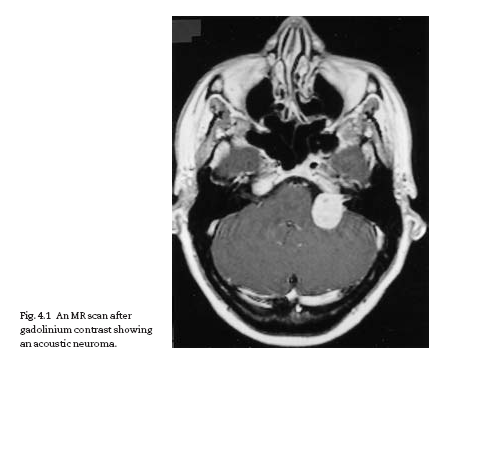
Vestibular Schwannoma (Acoustic neuroma)
Vestibular Schwannoma is a benign tumour of the superior vestibular nerve in
the internal auditory meatus or cerebello-pontine (CP) angle. It is usually
unilateral, except in familial neurofibromatosis (NF2), when it may be bilat-eral. In its early stages, it causes a progressive hearing loss and some imbalance.
As it enlarges, it may encroach on the trigeminal nerve in the CP angle,
causing loss of corneal sensation. In its advanced stage, there is raised intracranial
pressure and brain stem displacement. Early diagnosis reduces
the morbidity and mortality of operations. Unilateral sensorineural deafness
should always be investigated to exclude a neuroma. Audiometry will
confirm the hearing loss. MR scanning will identify even small tumours with
certainty (Fig. 4.1).
Hearing aids
In cochlear forms of sensorineural deafness, loudness recruitment is often
a marked feature. This results in an intolerance of noise above a certain
threshold, and makes the provision of amplification very difficult.
The choice of hearing aids is now large. Most are worn behind the ear
with a mould fitting into the meatus. If the mould does not fit well, oscillatory
feedback will occur and the patient will not wear the aid. More sophisticated
(and expensive) are the ‘all-in-the-ear’ aids, where the electronics
are built into a mould made to fit the patient’s ear. They give good directional
hearing and, because they are individually built, the output can bematched to the patient’s deafness. The current generation of hearing aids
are digital, allowing more refinement in the sound processing and more
control of the aid.
A recent development has been the bone-anchored hearing aid
(BAHA). A titanium screw is threaded into the temporal bone and allowed
to fuse to the bone (osseo-integration). A transcutaneous abutment then
allows the attachment of a special hearing aid that transmits sound directly
by bone conduction to the cochlea.The main application of BAHA is to patients
with no ear canal, or chronic ear disease, who are unable to wear a
conventional aid and is much more effective than the old-fashioned bone
conductor aid.
Cochlear implants
Much research has been done, both in the USA and Europe, on the implantation
of electrodes into the cochlea to stimulate the auditory nerve.The
apparatus consists of a microphone, an electronic sound processor and a
single or multichannel electrode implanted into the cochlea. Cochlear implantation
is only appropriate for the profoundly deaf. Results, particularly
with an intracochlear multichannel device, can be spectacular, with some
patients able to converse easily. Most patients obtain a significant improvement
in their ability to communicate and implantation has been extended
for use in children. It is no longer an experimental procedure but a valuable
therapeutic technique.
Lip-reading
Instruction in lip-reading is carried out much better while usable hearing
persists and should always be advised to those at risk of total or profound
deafness.
Electronic aids for the deaf
Amplifying telephones are easily available to the deaf and telephone companies
usually provide willing advice. Many modern hearing aids are fitted with
a loop inductance system to make the use of telephones easier.
Various computerized voice analysers that give a rapid visual display are
also available, but these require the services of a skilled operator and are
still in the developmental phase. Automatic voice recognition machines maytake over this role in the foreseeable future.


Download Files
Course Material
- The Ear: Some Applied Anatomy
- Clinical Examination of the Ear
- Testing the Hearing
- Deafness
- Conditions of the Pinna
- Conditions of the External Auditory Meatus
- Injury of the Tympanic Membrane
- Acute Otitis Media
- Chronic Otitis Media
- Complications of Middle-Ear Infection
- Otitis Media with Effusion
- Otosclerosis
- Earache (Otalgia)
- Vertigo
- Facial Nerve Paralysis
- Adenoids
- The Tonsils and Oropharynx
- Tonsillectomy
- Retropharyngeal Abscess
- Examination of the Larynx
- Injuries of the Larynx and Trachea
- Acute Disorders of the Larynx
- Chronic Disorders of the Larynx
- Tumours of the Larynx
- Vocal Cord Paralysis
- Airway Obstruction in Infants and Children
- Conditions of the Hypopharynx
- Tracheostomy
- Diseases of the Salivary Glands
- Chapters 29
- Department Sargodha Medical College
- Teacher
Dr. Muhammad Khalil
