
WEEK 20-25:REGULATION OF RESPIRATION
Respiratory Center
The respiratory center is composed of several groups of neurons located bilaterally
in the medulla oblongata and pons of the brain stemIt is divided into three major collections of neurons: (1) a dorsal respiratory
group, located in the dorsal portion of the medulla, which mainly causes
inspiration; (2) a ventral respiratory group, located in the ventrolateral part of
the medulla, which mainly causes expiration; and (3) the pneumotaxic center,
located dorsally in the superior portion of the pons, which mainly controls rate
and depth of breathing.The dorsal respiratory group of neurons plays the most
fundamental role in the control of respirationDorsal Respiratory Group of Neurons—Its Control
of Inspiration and of Respiratory Rhythm
The dorsal respiratory group of neurons extends most of the length of the
medulla. Most of its neurons are located within the nucleus of the tractus solitarius,
although additional neurons in the adjacent reticular substance of the
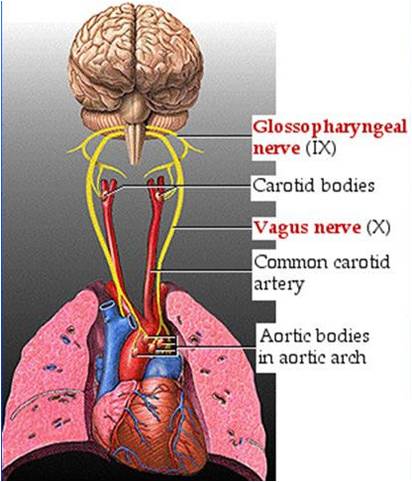
medulla also play important roles in respiratory control. The nucleus of the
tractus solitarius is the sensory termination of both the vagal and the glossopharyngeal
nerves, which transmit sensory signals into the respiratory center
from (1) peripheral chemoreceptors, (2) baroreceptors, and (3) several types of
receptors in the lungs.Ventral Respiratory Group of
Neurons—Functions in Both
Inspiration and Expiration
Located in each side of the medulla, about 5 millimeters
anterior and lateral to the dorsal respiratory group
of neurons, is the ventral respiratory group of neurons,
found in the nucleus ambiguus rostrally and the
nucleus retroambiguus caudally. The function of this
neuronal group differs from that of the dorsal respiratory
group in several important ways:
1. The neurons of the ventral respiratory group
remain almost totally inactive during normal quiet
respiration. Therefore, normal quiet breathing is
caused only by repetitive inspiratory signals from
the dorsal respiratory group transmitted mainly to
the diaphragm, and expiration results from elastic
recoil of the lungs and thoracic cage.
2. There is no evidence that the ventral respiratory
neurons participate in the basic rhythmical
oscillation that controls respiration.
3. When the respiratory drive for increased
pulmonary ventilation becomes greater than
normal, respiratory signals spill over into the
ventral respiratory neurons from the basic
oscillating mechanism of the dorsal respiratory
area. As a consequence, the ventral respiratory
area contributes extra respiratory drive as well.
4. Electrical stimulation of a few of the neurons in
the ventral group causes inspiration, whereas
stimulation of others causes expiration. Therefore,
these neurons contribute to both inspiration and
expiration. They are especially important in
providing the powerful expiratory signals to the
abdominal muscles during very heavy expiration.
Thus, this area operates more or less as an
overdrive mechanism when high levels of
pulmonary ventilation are required, especially
during heavy exercise.
Lung Inflation Signals Limit
Inspiration—The Hering-Breuer
Inflation Reflex
In addition to the central nervous system respiratory
control mechanisms operating entirely within the
brain stem, sensory nerve signals from the lungs also
Pneumotaxic center
Fourth ventricle
Dorsal respiratory
group (inspiration)
Vagus and
glossopharyngeal
? Apneustic center
Inhibits
Ventral respiratory
group (expiration
and inspiration)
Respiratory motor
pathway
Organization of the respiratory center.Chemical Control
of Respiration
The ultimate goal of respiration is to maintain proper
concentrations of oxygen, carbon dioxide, and hydrogen
ions in the tissues. It is fortunate, therefore, that
respiratory activity is highly responsive to changes in
each of these.
Excess carbon dioxide or excess hydrogen ions in
the blood mainly act directly on the respiratory center
itself, causing greatly increased strength of both the
inspiratory and the expiratory motor signals to the
respiratory muscles.
Oxygen, in contrast, does not have a significant
direct effect on the respiratory center of the brain in
controlling respiration. Instead, it acts almost entirely
on peripheral chemoreceptors located in the carotid
and aortic bodies, and these in turn transmit appropriate
nervous signals to the respiratory center for
control of respiration.
Let us discuss first the stimulation of the respiratory
center itself by carbon dioxide and hydrogen ionsOther Factors That
Affect Respiration
Voluntary Control of Respiration. Thus far, we have discussed
the involuntary system for the control of respiration.
However, we all know that for short periods of
time, respiration can be controlled voluntarily and that
one can hyperventilate or hypoventilate to such an
extent that serious derangements in Pco2, pH, and Po2
can occur in the blood.
Effect of Irritant Receptors in the Airways. The epithelium of
the trachea, bronchi, and bronchioles is supplied with
sensory nerve endings called pulmonary irritant receptors
that are stimulated by many incidents. These cause
coughing and sneezing, as discussed in Chapter 39.They
may also cause bronchial constriction in such diseases
as asthma and emphysema.
Function of Lung “J Receptors.” A few sensory nerve
endings have been described in the alveolar walls in
juxtaposition to the pulmonary capillaries—hence the
name “J receptors.”They are stimulated especially when
the pulmonary capillaries become engorged with blood
or when pulmonary edema occurs in such conditions as
congestive heart failure. Although the functional role of
the J receptors is not clear, their excitation may give the
person a feeling of dyspnea.
Effect of Brain Edema. The activity of the respiratory
center may be depressed or even inactivated by acute
brain edema resulting from brain concussion. For
instance, the head might be struck against some solid
object, after which the damaged brain tissues swell,
compressing the cerebral arteries against the cranial
vault and thus partially blocking cerebral blood supply.
Occasionally, respiratory depression resulting from
brain edema can be relieved temporarily by intravenous
injection of hypertonic solutions such as highly concentrated
mannitol solution. These solutions osmotically
remove some of the fluids of the brain, thus relievingAnesthesia. Perhaps the most prevalent cause of respiratory
depression and respiratory arrest is overdosage
with anesthetics or narcotics. For instance, sodium pentobarbital
depresses the respiratory center considerably
more than many other anesthetics, such as halothane.At
one time, morphine was used as an anesthetic, but this
drug is now used only as an adjunct to anesthetics
because it greatly depresses the respiratory center while
having less ability to anesthetize the cerebral cortex.
intracranial pressure and sometimes re-establishing respiration


Download Files
- Chapters 6
- Department Physiology
- Teacher
Dr. Madiha Nazir
