
PREGNANCY AND LACTATION
Maternal physiological changes in pregnancy are the adaptations during pregnancy that a woman's body undergoes to accommodate the growing embryo or fetus. These physiologic changes are entirely normal, and include behavioral (brain), cardiovascular(heart and blood vessel), hematologic (blood), metabolic, renal (kidney), posture, and respiratory (breathing) changes. Increases in blood sugar, breathing, and cardiac output are all expected changes that allow a pregnant woman's body to facilitate the proper growth and development of the embryo or fetus during the pregnancy. The pregnant woman and the placenta also produce many other hormones that have a broad range of effects during the pregnancy.
Levels of progesterone and estrogen rise continually throughout pregnancy, suppressing the hypothalamic axis and subsequently the menstrual cycle. The progesterone is first produced by the corpus luteum and then by the placenta in the second trimester. Women also experience increased human chorionic gonadotropin (β-hCG), which is produced by the placenta.
Lactation
Lactation is the maternal physiological response whereby milk is secreted from the mammary glands to feed the infant. In this article we will cover the synthesis and regulation of milk production and also the let-down reflex that releases milk.
The mammary glands are embedded in the breasts. The mammary gland comprises 15-20 lobulated masses of tissue with fibrous tissue connecting the lobes and adipose tissue in between. The lobes are made up of alveoli, blood vessels and lactiferous ducts. At birth there are only a few ducts present and at puberty oestrogen causes the ducts to sprout and the ends form masses of cells that later become alveoli.
With each menstrual cycle there are cyclic changes due to changes in oestrogen and progesterone.
During pregnancy there is significant hypertrophy of the ductular-lobular-alveolar system, prominent lobules form and from mid-gestation alveolar cells differentiate to be capable of milk production. During pregnancy there is little milk secretion due to the highprogesterone : oestrogen ratio which favours growth rather than secretion.
Regulation of Milk Production
Regulation of quantity and content of milk is largely under hormonal control, primarily prolactin.
During pregnancy, a high progesterone : oestrogen ratio favours the development of alveoli, but not secretion. With the delivery of the placenta, the source of the large amount of circulating steroids (more so progesterone) is removed allowing the alveoli to respond to prolactin. Breast milk begins to form within 24 – 48 hours.
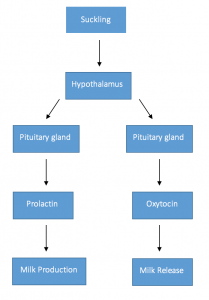
Prolactin is a polypeptide hormone and is secreted by the anterior pituitary gland. This is controlled by dopamine (also known as Prolactin Inhibiting Hormone) from the hypothalamus (inhibits prolactin). Factors promoting secretion of prolactin reduce dopamine secretion in a negative feedback loop. It is also produced by decidual cells.
Prolactin stimulation is promoted by suckling and is a neuro-endocrine reflex. Suckling mechanically stimulates receptors in the nipple and impulses pass up to the brain stem and to the hypothalamus to reduce the secretion of dopamine and increase vasoactive intestinal protein (promotes prolactin secretion). Suckling at one feed promotes prolactin release which causes production for the next feed which accumulates in alveoli and ducts (turgor).
Milk Let-Down Reflex
Mechanical stimulation of nipple is responsible for milk delivery to infant and maintenance of lactation. Babies do not suck the milk out of the breast, it is ejected by the let-down reflex. In response to suckling, oxytocin is released from the pituitary gland which stimulates myoepithelial cells that surround alveoli to contract thus squeezing milk out of the breast.
Maintaining Milk Production
The key to maintaining milk production is sufficient suckling stimulation at each feed to maintain prolactin secretion and to remove accumulated milk. If suckling stops, milk production ceases gradually. This is due to turgor induced damage to secretory cells and low prolactin levels. Milk suppression can also be achieved via steroids.
Prolactin secretion during lactation reduces fertility and so makes a new pregnancy less likely until the infant stops suckling.
By the end of this lecture students should know about
- maturation and fertilisation of ovum
- functions of placenta
- hormones produced by placenta
- lactation and let down reflex


Download Files
Course Material
- Chapters 4
- Department Physiology
- Teacher
Dr. Faryal Mazhar
