
Week 10: Social Cognitive Theory
Social Cognitive Theory
Introduction
Social Cognitive Theory (SCT) started as the Social Learning Theory (SLT) in the 1960s by Albert Bandura. It developed into the SCT in 1986 and posits that learning occurs in a social context with a dynamic and reciprocal interaction of the person, environment, and behavior. The unique feature of SCT is the emphasis on social influence and its emphasis on external and internal social reinforcement. SCT considers the unique way in which individuals acquire and maintain behavior, while also considering the social environment in which individuals perform the behavior. The theory takes into account a person's past experiences, which factor into whether behavioral action will occur. These past experiences influences reinforcements, expectations, and expectancies, all of which shape whether a person will engage in a specific behavior and the reasons why a person engages in that behavior.
Many theories of behavior used in health promotion do not consider maintenance of behavior, but rather focus on initiating behavior. This is unfortunate as maintenance of behavior, and not just initiation of behavior, is the true goal in public health. The goal of SCT is to explain how people regulate their behavior through control and reinforcement to achieve goal-directed behavior that can be maintained over time. The first five constructs were developed as part of the SLT; the construct of self-efficacy was added when the theory evolved into SCT.
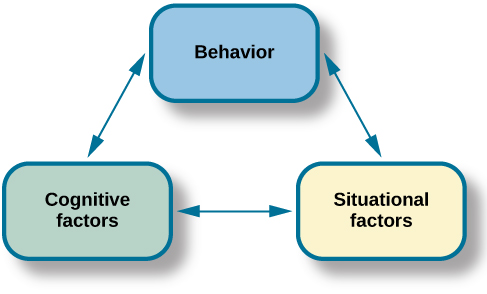
- Reciprocal Determinism - This is the central concept of SCT. This refers to the dynamic and reciprocal interaction of person (individual with a set of learned experiences), environment (external social context), and behavior (responses to stimuli to achieve goals).
- Behavioral Capability - This refers to a person's actual ability to perform a behavior through essential knowledge and skills. In order to successfully perform a behavior, a person must know what to do and how to do it. People learn from the consequences of their behavior, which also affects the environment in which they live.
- Observational Learning - This asserts that people can witness and observe a behavior conducted by others, and then reproduce those actions. This is often exhibited through "modeling" of behaviors. If individuals see successful demonstration of a behavior, they can also complete the behavior successfully.
- Reinforcements - This refers to the internal or external responses to a person's behavior that affect the likelihood of continuing or discontinuing the behavior. Reinforcements can be self-initiated or in the environment, and reinforcements can be positive or negative. This is the construct of SCT that most closely ties to the reciprocal relationship between behavior and environment.
- Expectations - This refers to the anticipated consequences of a person's behavior. Outcome expectations can be health-related or not health-related. People anticipate the consequences of their actions before engaging in the behavior, and these anticipated consequences can influence successful completion of the behavior. Expectations derive largely from previous experience. While expectancies also derive from previous experience, expectancies focus on the value that is placed on the outcome and are subjective to the individual.
- Self-efficacy - This refers to the level of a person's confidence in his or her ability to successfully perform a behavior. Self-efficacy is unique to SCT although other theories have added this construct at later dates, such as the Theory of Planned Behavior. Self-efficacy is influenced by a person's specific capabilities and other individual factors, as well as by environmental factors (barriers and facilitators).
Capacities
Evolving over time, human beings are featured with advanced neural systems, which enable individuals to acquire knowledge and skills by both direct and symbolic terms.[2] Four primary capabilities are addressed as important foundations of social cognitive theory: symbolizing capability, self-regulation capability, self-reflective capability, and vicarious capability.
- Symbolizing Capability: People are affected not only by direct experience but also indirect events. Instead of merely learning through laborious trial-and-error process, human beings are able to symbolically perceive events conveyed in messages, construct possible solutions, and evaluate the anticipated outcomes.
- Self-regulation Capability: Individuals can regulate their own intentions and behaviors by themselves. Self-regulation lies on both negative and positive feedback systems, in which discrepancy reduction and discrepancy production are involved. That is, individuals proactively motivate and guide their actions by setting challenging goals and then making effort to fulfill them. In doing so, individuals gain skills, resources, self-efficacy and beyond.
- Self-reflective Capability: Human beings can evaluate their thoughts and actions by themselves, which is identified as another distinct feature of human beings. By verifying the adequacy and soundness of their thoughts through enactive, various, social, or logical manner, individuals can generate new ideas, adjust their thoughts, and take actions accordingly.
- Vicarious Capability: One critical ability human beings feature is the ability to adopt skills and knowledge from information communicated through a wide array of mediums. By vicariously observing others’ actions and their consequences, individuals can gain insights into their own activities. Vicarious capability is of great value to human beings’ cognitive development in nowadays, in which most of our information encountered in our lives derives from the mass media than trial-and-error processes.
Limitation of Social Cognitive Theory
There are several limitations of SCT, which should be considered when using this theory in public health. Limitations of the model include the following:
- The theory assumes that changes in the environment will automatically lead to changes in the person, when this may not always be true.
- The theory is loosely organized, based solely on the dynamic interplay between person, behavior, and environment. It is unclear the extent to which each of these factors into actual behavior and if one is more influential than another.
- The theory heavily focuses on processes of learning and in doing so disregards biological and hormonal predispositions that may influence behaviors, regardless of past experience and expectations.
- The theory does not focus on emotion or motivation, other than through reference to past experience. There is minimal attention on these factors.
- The theory can be broad-reaching, so can be difficult to operationalize in entirety.
Social Cognitive Theory considers many levels of the social ecological model in addressing behavior change of individuals. SCT has been widely used in health promotion given the emphasis on the individual and the environment, the latter of which has become a major point of focus in recent years for health promotion activities. As with other theories, applicability of all the constructs of SCT to one public health problem may be difficult especially in developing focused public health programs.


- Week 1: Uses and Gratification Theory
- Week 2: Agenda Setting Theory
- Week 3: Cultivation Theory
- Week 4: Diffusion of Innovation Theory
- Week 5: Knowledge Gap Theory
- Week 6: Social Learning Theory
- Week 7: Media Effects
- Week 8: Gatekeeping Theory
- Week 9: Propaganda Model
- Week 10: Social Cognitive Theory
- Week 11: Rhetoric Model of Persuasion
- Week 12: Elaboration Likelihood Model
- Week 13: Table of Theories (Timeline)
- Week 14: Categorization of Theories
- Week 15: Theories Task 1
- Week 16: Theories Task 2
- Chapters 16
- Department Communication and Media Studies
- Teacher
Zowaina Azhar
